Home › Biological sample › Cancer › Colorectal
Colorectal cancer biological samples
For Research Applications
Creating drugs and diagnostic tests for treating and detecting colorectal cancer necessitates conducting studies on biological samples collected from patients with the disease.
A brief overview of the various colorectal cancer types and how the services offered by Labtoo contribute to accelerating research and development projects in the pharmaceutical industry.

Biospecimen from colorectal cancer patients
Tissues from colorectal cancer patients (tumoral & normal adjacent)
Fresh resection & biopsy
Frozen samples (OCT & FF)
FFPE blocks & slides
Blood derivatives from colorectal cancer patients
-
Whole Blood
-
PBMC
-
Plasma
-
Serum
Biofluids from colorectal cancer patients
-
Feces
-
Urine
-
Ascite
-
Other
Associated clinical data from colorectal cancer patients
-
Age
-
Gender
-
TNM Classification
-
Undergone Treatment
-
Medical Imaging
-
HIV/HBV/HCV status
-
Mutations
-
Other Data (upon request)
Send your request to our team:
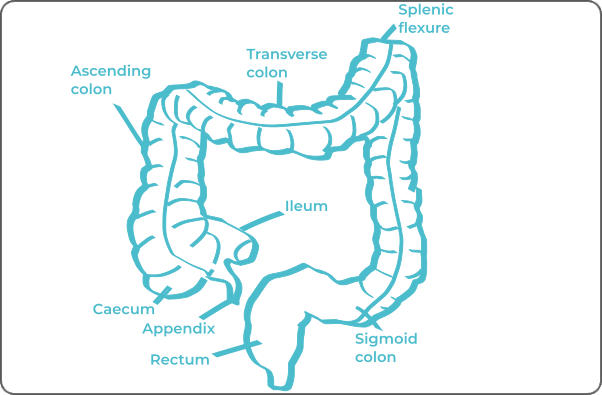
What are colorectal tumors?
Colorectal cancer encompasses various tumors that can form from the colon to the rectum. Generally, two-thirds of colorectal cancers originate in the colon, with the remaining one-third arising from the rectum.
In 80% of cases, these cancers develop from adenomatous polyps, also known as adenomas or polyps, which are benign, non-cancerous tumors on the mucous membrane of the colon.
The vast majority of cancerous tumors are gastric adenocarcinomas (or gastric carcinomas) that form from the glandular epithelial cells of the colon or rectum mucosa. Adenocarcinomas can be classified into different subcategories based on the level of differentiation, cell morphology, and mucin production. Notably, Lieberkühn adenocarcinoma and mucinous adenocarcinoma are distinguished among them.
Colorectal cancers have the ability to metastasize. When this occurs, they tend to spread primarily to the liver and lungs, and to a lesser extent, to lymph nodes, bones, and the peritoneum.
| Colorectal Cancer Type | Originating Cell | Frequency |
|---|---|---|
| Lieberkühn Adenocarcinoma | Glandular Cell | ≈ 85% |
| Mucinous Adenocarcinoma | Glandular Cells | ≈ 10% |
| Squamous Cell Carcinoma | Squamous Cell | Rare |
| Colorectal Carcinoid Tumor | Neuroendocrine Cell | >1% |
| Anal Canal Melanoma | Melanocyte | Rare |
| Gastrointestinal Stromal Tumor (GIST) | Mesenchymal Cell | 1 - 3% of gastrointestinal tumors |
Explore Labtoo's Service for Your Biological Sample Research
Labtoo assists you in sourcing biological samples from colorectal cancer patients. Our team manages the entire project of transferring biological materials from inception to sample delivery.
- Feasibility assessment of sample availability or clinical collection from referenced clinical centers
- Validation of regulatory aspects
- Establishment of a contractual framework
- Dispatch of desired samples under appropriate conditions
- Transfer of associated clinical data
- Additional analytical and experimental services
Genetic Mutations Involved in Colorectal Cancer
Scientific research has identified a number of genetic mutations associated with an increased risk of colorectal cancer. These mutations often affect genes responsible for DNA repair, cellular signaling, and tumor suppression. Key genes implicated include:
- APC
- BMPR1A
- EPCAM
- MLH1
- MSH2 and MSH6
- PMS2
- CHEK2
- POLE
- PTEN
- SMAD4
- STK11
- TP53
- MUTYH
These mutations can be inherited or acquired and play a critical role in the development and progression of colorectal cancer. Genetic testing enables the detection of these abnormalities, providing valuable insights for risk assessment and personalized therapeutic approaches.
The stages and grades of colorectal cancer
The stage and grade of cancer are commonly used together to provide a comprehensive assessment of the disease and guide optimal treatment.
The determination of cancer stage relies primarily on the TNM classification, evaluating the size of the tumor (T), involvement of lymph nodes by cancer cells (N), and the presence of metastases in other parts of the body (M).
In parallel, the grade provides an indication of the degree of differentiation of cancer cells, often ranging between 1 and 3.
For colorectal cancer, the stages are represented as follows:
Stage 0
Presence of cancer cells confined to the colorectal mucosa (carcinoma in situ).
Stage I
Invasion of the connective tissue layer surrounding the mucosa, either at the submucosal or muscular layer.
Stage II
The tumor may invade the tissue layer between the muscular and serosal layers.
It may also penetrate the membrane supporting the colon and rectum (visceral peritoneum) or breach the wall of the colon or rectum to reach other organs such as the prostate, bladder, or uterus.
Stage III
Presence of metastases in lymph nodes near the colorectal system.
Stage IV
Development of metastases that have spread to other organs, distant lymph nodes, or the peritoneum.
Rare forms of colorectal cancer
Occasionally, rare forms of colorectal cancer develop, among which are:
-
Squamous Cell Carcinoma
A rare cancer that develops from squamous cells.
-
Colorectal Carcinoid Tumor
A rare cancer that develops from neuroendocrine cells.
-
Gastrointestinal Stromal Tumors (GISTs)
Gastrointestinal Stromal Sarcomas are rare cancers that develop from cells of the connective tissue called stroma in the wall of the gastrointestinal tract.
-
Melanoma
A rare cancer that develops from melanocytes in the anal canal.
Colorectal cancer treatments and advances
Treatment for brain cancer relies on a multimodal approach, where surgery, often assisted by imaging tools, is commonly used for tumor removal. In addition to surgery, several methods are applied.
-
Chemotherapy: Often used when there is lymph node involvement. The method employs anticancer agents such as 5-fluorouracil.
-
Radiotherapy: Involves destroying cancer cells using ionizing radiation. Frequently used to treat rectal cancers, it often precedes surgery and may be complemented by chemotherapy.
-
Targeted Therapy: An emerging option targeting specific molecules in the tumor. For colorectal cancer, two types of treatment are used – anti-angiogenics blocking tumor angiogenesis and anti-Epidermal Growth Factor receptors preventing proliferation.
-
Immunotherapy: A relatively recent method that stimulates the patient's immune system to enhance its ability to recognize and destroy cancer cells. The use of immunotherapy for colorectal cancer has made significant advances but is not yet universally widespread.
The choice of treatment depends on the specific type of cancer, the stage of the disease, and other individual factors, all aimed at optimizing the chances of remission.

Additional resources


