Home › Biological sample › Cancer › Esophageal
Esophageal cancer biological samples
For Research Applications
The development of drugs and diagnostic tests for the treatment and detection of esophageal cancer requires conducting studies on biological samples obtained from patients with esophageal cancer.
A brief overview of the various types of esophageal cancer and how the services offered by Labtoo contribute to accelerating research and development projects in the pharmaceutical industry.

Biospecimen from esophageal cancer patients
Tissues from esophageal cancer patients (tumoral & normal adjacent)
Fresh resection & biopsy
Frozen samples (OCT & FF)
FFPE blocks & slides
Blood derivatives from esophageal cancer patients
-
Whole Blood
-
PBMC
-
Plasma
-
Serum
Biofluids from esophageal cancer patients
-
Esophageal lavage
-
Urine
-
Other
Associated clinical data from esophageal cancer patients
-
Age
-
Gender
-
TNM Classification
-
Undergone Treatment
-
Medical Imaging
-
HIV/HBV/HCV status
-
Mutations
-
Other Data (upon request)
Send your request to our team:
What are esophageal tumors?
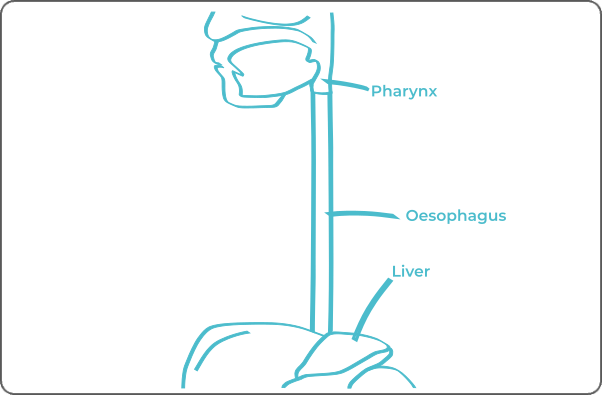
The esophagus, a musculo-membranous structure of the digestive system, plays a pivotal role in efficiently transporting ingested food from the mouth to the stomach, facilitated by muscular contractions. Comprising both striated and smooth muscle tissue, along with a protective mucosal lining, the esophagus exhibits a specific anatomical structure enabling effective propulsion of food particles while serving as a barrier against potential aggressions.
There are two common types of esophageal cancer: Squamous cell carcinoma and adenocarcinoma. The proportion of these cancer types varies significantly across geographical regions. Historically, globally, squamous cell carcinoma of the esophagus has been more prevalent than adenocarcinoma.
Squamous cell carcinoma
The origin of esophageal squamous cell carcinoma lies in the malignant transformation of squamous cells in the esophageal mucosa, primarily localized in its upper portion.
This pathology is frequently associated with risk behaviors such as excessive alcohol consumption and smoking.
In France, squamous cell carcinoma predominates, accounting for approximately 75% of cases, a prevalence that notably differs from the trend observed in most other Western nations.
Adenocarcinoma
Adenocarcinoma originates in the lower region of the esophagus, arising from flat squamous cells of the mucosa that have undergone transformation into glandular cells.
This transformation occurs through Barrett's metaplasia, an adaptive response to lesions often induced by chronic gastroesophageal reflux.
Among the predominant risk factors, diet plays a significant role in the development of this type of cancer.
Although its incidence has been steadily increasing in the West in recent years, adenocarcinoma is more common in the United States and Canada, where it predominates, compared to the situation observed in France.
| Type of Esophageal Cancer | Originating Cell | Frequency |
|---|---|---|
| Squamous Cell Carcinoma | Squamous cell | Prevalent, varies greatly by geographical regions |
| Adenocarcinoma | Glandular cell | Varies greatly by geographical regions |
| Leiomyosarcoma | Connective or muscular tissue cell of the esophagus | Rare |
| Neuroendocrine Carcinoma | Neuroendocrine cell of the esophagus | Rare |
| Gastrointestinal Stromal Tumor | Stromal cell of the esophagus | Rare |
Esophageal cancer has the capacity to metastasize, spreading to other parts of the body. The most common sites of metastasis for esophageal cancer often include local lymph nodes, the liver, lungs, and occasionally the bones.

Explore Labtoo's Service for Your Biological Sample Research
Labtoo assists you in sourcing biological samples from esophageal cancer patients. Our team manages the entire project of transferring biological materials from inception to sample delivery.
- Feasibility assessment of sample availability or clinical collection from referenced clinical centers
- Validation of regulatory aspects
- Establishment of a contractual framework
- Dispatch of desired samples under appropriate conditions
- Transfer of associated clinical data
- Additional analytical and experimental services
The stages and grades of esophageal cancer
The stage and grade of cancer are commonly used together to provide a comprehensive assessment of the disease and guide treatment optimally.
The determination of cancer stage primarily relies on the TNM classification, which evaluates the tumor size (T), involvement of lymph nodes by cancer cells (N), and presence of metastases in other parts of the body (M). Concurrently, the grade provides an indication of the degree of differentiation of cancer cells.
Regarding grades, graded from 1 to 3, grade G1 indicates well-differentiated cells resembling normal cells, grade G2 represents moderately differentiated cells, and grade G3 indicates poorly differentiated cells, suggesting faster growth and potentially more aggressive behavior.
As for the stages of esophageal cancer, they are represented as follows:
Stage 0
The tumor remains within the epithelium of the inner lining of the esophagus.
This is referred to as carcinoma in situ.
Stage I
The tumor has invaded the deeper layers of the esophageal wall.
The tumor has not spread to lymph nodes or other parts of the body.
Stage I A
Invasion of the mucosa or submucosa.
Stage I B
Invasion of the muscularis.
Stage II
Invasion of the deep layer of the wall (adventitia) or involvement of up to two adjacent lymph nodes.
No spread to other parts of the body.
Stage II A
Invasion of the adventitia.
No spread to lymph nodes.
Stage II B
The tumor has invaded the mucosa, submucosa, or muscular layer, and at most, two neighboring lymph nodes are affected.
Stage III
The tumor involves more than two lymph nodes or has begun to invade neighboring tissues.
No spread to other parts of the body.
Stage III A
Either the tumor has invaded the pleura, pericardium, or diaphragm without spreading to lymph nodes.
Or the tumor has invaded the adventitia and one or two neighboring lymph nodes.
Or the tumor has invaded the mucosa, submucosa, or muscular layer and also involves 3 to 6 lymph nodes.
Stage III B
The tumor has invaded the adventitia and has affected between 3 and 6 lymph nodes.
Stage III C
Either the tumor has invaded the pleura, pericardium, or diaphragm, and 1 to 6 lymph nodes are affected.
Or it has invaded neighboring tissues such as the aorta, trachea, or a vertebra.
Or more than 6 lymph nodes are affected.
Stage IV
The tumor has spread to other parts of the body.
Rare forms of esophageal cancer
Rare forms of esophageal cancer may arise, among them are:
-
Leiomyosarcomas
Esophageal leiomyosarcoma is a rare form of cancer that develops from the smooth muscle cells of the esophageal wall. These tumors are classified as sarcomas. Due to its rarity, esophageal leiomyosarcoma presents particular diagnostic and therapeutic challenges.
-
Neuroendocrine Carcinomas
Esophageal neuroendocrine carcinoma is a rare form of cancer that develops from neuroendocrine cells present in the esophageal mucosa. These cells produce and release hormones, and their malignant transformation can lead to tumor formation.
-
Gastrointestinal Stromal Tumors
Rare neoplasms that form in the connective tissue of the esophageal wall. These tumors typically originate from interstitial cells of Cajal, which regulate the muscular movements of the esophagus.
Esophageal cancer treatments and advances
The treatment of esophageal cancer depends on the type of cancer, its stage, and the patient's physical condition. The main therapeutic modalities include surgery, radiotherapy, chemotherapy, immunotherapy, and targeted therapies.
-
Surgery: Surgery, including esophagectomy, is commonly recommended. It involves the resection of part or all of the esophagus, depending on the stage of the disease.
-
Radiotherapy: Using radiation, conformal external beam radiotherapy is frequently administered, especially in cases of squamous cell carcinoma of the esophagus. It can be delivered as monotherapy or in conjunction with chemotherapy.
-
Chemotherapy: Often combined with radiotherapy, chemotherapy is used in the preoperative or postoperative setting. In cases of recurrence or ineligibility for surgical intervention, chemotherapy alone may be considered.
-
Immunotherapy: By stimulating the immune system, immunotherapy is increasingly integrated into the treatment of esophageal cancer, often in combination with chemotherapy.
- Targeted Therapies: These drugs target specific abnormalities present in cancer cells, focusing on identified genetic mutations. In the case of esophageal cancer, they may target the HER2 receptor (when present) with trastuzumab or inhibit angiogenesis with ramucirumab.

Additional resources