Home › Biological sample › Cancer › Kidney
Kidney cancer biological samples
For research applications
The development of drugs and diagnostic tests for the treatment and detection of kidney cancer requires conducting studies on biological samples obtained from patients with kidney cancer.
A brief overview of the various kidney cancer types and how the services offered by Labtoo contribute to accelerating research and development projects in the pharmaceutical industry.

Biospecimen from kidney cancer patients
Tissues from kidney cancer patients (tumoral & normal adjacent)
Fresh resection & biopsy
Frozen samples (OCT & FF)
FFPE blocks & slides
Blood derivatives from kidney cancer patients
-
Whole Blood
-
PBMC
-
Plasma
-
Serum
Biofluids from kidney cancer patients
-
Urine
-
Other
Associated clinical data from kidney cancer patients
-
Age
-
Gender
-
TNM Classification
-
Undergone Treatment
-
Medical Imaging
-
HIV/HBV/HCV status
-
Mutations
-
Other Data (upon request)
Send your request to our team:
What are kidney tumors?
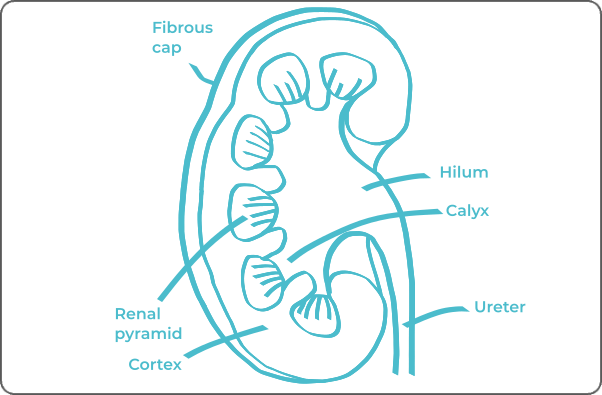
Renal cancers, or nephrocarcinomas, primarily arise from the renal parenchymal cells, which encompass the fundamental structures responsible for various organ functions such as regulating water and mineral substances in the blood, hormone production, and red blood cell precursor generation.
The classification of renal cancers generally relies on their histological form, meaning their appearance under the microscope. Two main subgroups are distinguished: clear cell carcinomas (or clear cell adenocarcinomas) and non-clear cell carcinomas (or non-clear cell adenocarcinomas).
Clear cell carcinomas
They are the most common, representing nearly 75% of renal cancers.
They typically originate from the proximal tubular cells of the kidney, which are involved in blood filtration to form urine.
Their clear appearance under the microscope is due to the presence of lipids and glycogen.
Non-clear cell carcinomas
They are less common. Unlike clear cell carcinoma, non-clear cell renal carcinoma (NCCR) can develop from various types of renal cells. Non-clear cell carcinomas encompass several subtypes of renal tumors including:
Papillary carcinoma, constituting approximately 15% of renal cancers. Cancerous cells exhibit a "finger-like" configuration.
Chromophobe carcinoma is characterized by large cells of pale brown color. Although rare , it is considered to be low-aggressive, low-grade, and limited-stage, with a favorable prognosis.
Medullary carcinoma, extremely rare, is distinguished by increased aggressiveness and a tendency to metastasize more than other types of renal cancer. It is often associated with young adults carrying the sickle cell trait or suffering from sickle cell disease.
| Type of Kidney Cancer | Cell of Origin | Frequency |
|---|---|---|
| Clear Cell Carcinoma | Parenchymal cells (clear appearance under microscope) | ≈ 75% |
| Papillary Carcinoma | Renal parenchymal cells (finger-like appearance) | ≈ 15% |
| Chromophobe Carcinoma | Renal parenchymal cells (pale brown color) | ≈ 5% |
| Medullary Carcinoma | Parenchymal cells | ≈ 1% |
| Collecting Duct Carcinoma | Collecting duct cells | Rare |
| Renal Pelvis Cancer | Lining cells of the renal pelvis | Rare |
| Multilocular Cystic Carcinoma | Wall cells of renal cysts | Rare |
Some renal cancers have the ability to metastasize, mainly affecting lymph nodes in the abdominal region, lungs, and spine.

Explore Labtoo's Service for Your Biological Sample Research
Labtoo assists you in sourcing biological samples from kidney cancer patients. Our team manages the entire project of transferring biological materials from inception to sample delivery.
- Feasibility assessment of sample availability or clinical collection from referenced clinical centers
- Validation of regulatory aspects
- Establishment of a contractual framework
- Dispatch of desired samples under appropriate conditions
- Transfer of associated clinical data
- Additional analytical and experimental services
The stages and grades of kidney cancer
The stage and grade of cancer are commonly used in tandem to provide a comprehensive assessment of the disease and guide optimal treatment strategies.
The determination of cancer stage primarily relies on the TNM classification, which assesses the tumor size (T), involvement of lymph nodes by cancer cells (N), and the presence of metastases in other parts of the body (M). Simultaneously, the grade provides insight into the degree of differentiation of cancer cells.
Regarding grades, rated from 1 to 3, G1 indicates well-differentiated cells resembling normal cells, G2 represents moderately differentiated cells, and G3 indicates poorly differentiated cells, suggesting faster and potentially more aggressive growth.
As for the stages of kidney cancer, they are represented as follows:
Stage I
At this stage, the tumor remains localized within the kidney and does not exceed 7 centimeters in size.
Stage II
The tumor persists to be confined within the kidney, but its size exceeds 7 centimeters.
Stage III
This phase is characterized by two possibilities:
either an expansion of the tumor beyond the kidney, involving adjacent veins or perirenal adipose tissue,
Or the presence of metastases in nearby lymph nodes.
Stage IV
At this advanced stage, two scenarios are conceivable:
Tumor penetrates the fibrous tissue enveloping the kidney, potentially reaching the adrenal gland
Cancer spreads to distant regions of the body, generating distant metastases.
Rare forms of kidney cancer
It happens that rarer forms of kidney cancer may develop, among them:
-
Collecting Duct Carcinoma
This cancer type, also known as Bellini's carcinoma, arises from the cells of the epithelium of the collecting ducts, which facilitate the transport of urine from nephrons to renal calices. Its highly aggressive nature categorizes it as a malignant form necessitating specific management.
-
Renal Pelvis Cancer
Emerging from cells of the renal pelvis or ureters, this cancer originates within the renal collecting system. Precise characterization and appropriate management depend on the exact location of the tumor.
-
Multilocular Cystic Carcinoma
These distinctive carcinomas take shape from cells lining the walls of renal cysts. Often associated with a favorable prognosis, the survival rate is generally high.
-
Renal Sarcoma
This tumor type originates from the mesenchymal cells of the kidneys. Distinguished categories include leiomyosarcoma, developing from smooth muscle cells of the kidney, and stromal sarcoma, formed from the supporting tissue of the kidney.
Kidney cancer treatments and advances
The treatment of kidney cancer relies on several factors, including the cancer type, its stage, and the patient's physical condition. The main therapeutic modalities include:
-
Surgery: This method predominates when the cancer is localized or locally advanced. Partial nephrectomy is performed to remove the affected region, while total nephrectomy is conducted if the tumor is extensive.
-
Radiotherapy: Limitedly used, primarily in cases of advanced tumors for palliative purposes.
-
Chemotherapy: Rarely offered to kidney cancer patients, as renal tumors typically exhibit resistance to chemotherapy drugs.
-
Immunotherapy: The use of interleukin-2 and interferon-alpha is reserved for highly specific cases, such as lung metastases. However, it is gradually being replaced by targeted therapies.
-
Targeted Therapies: These drugs specifically target anomalies present in cancer cells. They are administered when specific genetic mutations are identified. For kidney cancer, antiangiogenic treatments and mTOR inhibitors are widely favored.
Regarding small tumors in inoperable patients, minimally invasive treatments like cryoablation or radiofrequency treatment may be recommended. These approaches provide effective alternatives while minimizing the invasiveness of the treatment.

Additional resources


