Home › Biological sample › Cancer › Head&Neck
Head & Neck cancer biological samples
For research applications
The development of drugs and diagnostic tests for the treatment and detection of head & neck cancer requires conducting studies on biological samples obtained from patients with head & neck cancer.
A brief overview of the various types of head & neck cancer and how the services offered by Labtoo contribute to accelerating research and development projects in the pharmaceutical industry.

Biospecimen from head & neck cancer patients
Tissues from head & neck cancer patients (tumoral & normal adjacent)
Fresh resection & biopsy
Frozen samples (OCT & FF)
FFPE blocks & slides
Blood derivatives from head & neck cancer patients
-
Whole Blood
-
PBMC
-
Plasma
-
Serum
Biofluids from head & neck cancer patients
-
Saliva
-
Urine
-
Swab
-
Other
Associated clinical data from head & neck cancer patients
-
Age
-
Gender
-
TNM Classification
-
Undergone Treatment
-
Medical Imaging
-
HIV/HBV/HCV status
-
Mutations
-
Other Data (upon request)
Send your request to our team:
What are head & neck tumors?
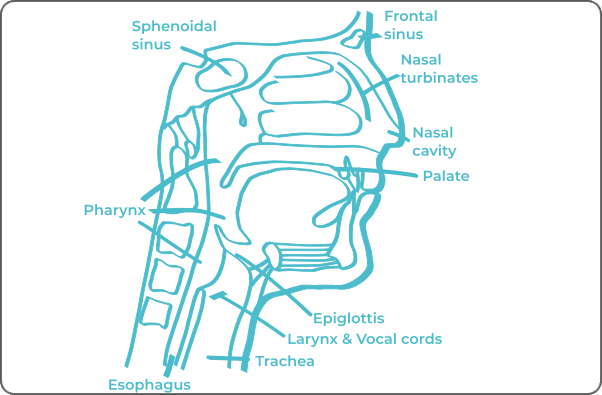
Cancers of the upper aerodigestive tract, commonly referred to as Head and Neck Cancers (HNC), encompass a spectrum of cancers that can develop in the head and neck region. These locations include the oral cavity, sinuses, nasopharynx, and larynx. Predominant risk factors associated with these cancers are primarily smoking and alcohol consumption. It is noteworthy that there is a correlation between the occurrence of oropharyngeal cancer and infection with the human papillomavirus (HPV).
In about 90% of cases, the tumor originates from the cells of the superficial layer of a mucous membrane, thereby characterizing squamous cell carcinoma.
Other types of tumors may arise from glandular cells. An illustrative example is adenocarcinoma of the pharynx, as well as those affecting the salivary glands.
The most frequently affected areas by HNC are as follows:
The mouth and pharynx
Accounting for approximately 75% of cases.
The larynx
Involved in about 30% of cases.
The nasopharynx and nasal fossae
Observed in about 2% of cases.
The sinuses of the face
With an incidence of about 0.1%.
| Type of Tumor | Cell of Origin | Frequency |
|---|---|---|
| Squamous Cell Carcinoma | Epithelial cells | ≈ 90% |
| Adenocarcinoma | Glandular cells | Rare |
| Adenoid Cystic Carcinoma | Glandular cells | Rare |
| Basal Cell Carcinoma of Mucosa | Basal cells | Rare |
| Small Cell Carcinoma | Neuroendocrine cells | Rare |
| Verrucous Squamous Cell Carcinoma | Epithelial cells | Rare |
| Spindle Cell Carcinoma | Epithelial cells | Rare |
Less common manifestations, such as sarcomas or undifferentiated cell tumors, can also emerge in the context of HNC.
The ability to metastasize is an inherent characteristic of HNC. Predominant metastatic sites generally include regional lymph nodes, lungs, liver, and other organs in the thoracic region.

Explore Labtoo's Service for Your Biological Sample Research
Labtoo assists you in sourcing biological samples from head&neck cancer patients. Our team manages the entire project of transferring biological materials from inception to sample delivery.
- Feasibility assessment of sample availability or clinical collection from referenced clinical centers
- Validation of regulatory aspects
- Establishment of a contractual framework
- Dispatch of desired samples under appropriate conditions
- Transfer of associated clinical data
- Additional analytical and experimental services
The stages and grades of head and neck cancers
The stage and grade of cancer are commonly used together to provide a comprehensive assessment of the disease and guide optimal treatment.
The determination of the cancer stage primarily relies on the TNM classification, which assesses the tumor size (T), involvement of lymph nodes by cancer cells (N), and the presence of metastases in other parts of the body (M).
Simultaneously, the grade provides an indication of the degree of differentiation of cancer cells. Noted from 1 to 3, grade G1 indicates well-differentiated cells resembling normal cells, grade G2 represents moderately differentiated cells, and grade G3 indicates poorly differentiated cells, suggesting faster and potentially more aggressive growth.
Head & neck cancers, as a diverse group of cancers, exhibit variations in their specific stages. However, here is a generic representation that can be applied:
Stage I
The tumor is confined to the original region, with no spread to nearby lymph nodes or other parts of the body.
Stage II
The tumor is more extensive or has slightly reached nearby lymph nodes while generally remaining confined to the original region.
Stage III
The tumor has significantly spread locally, possibly invading adjacent structures such as muscles, bones, or neighboring structures.
It may also affect lymph nodes.
Stage IV
At this advanced stage, the tumor has often invaded significant structures, may have extended its reach to distant lymph nodes, and may have generated metastases in other parts of the body, such as the lungs.
It is crucial to note that this classification provides an overview, and each individual case should be evaluated by a healthcare professional for an accurate determination of head & neck cancer stage.
Rare forms of head & neck cancer
It happens that rarer forms of kidney cancer develop, among them are:
-
Small Cell Carcinoma
Small cell carcinoma is a tumor that often originates from cells with neuroendocrine characteristics. This tumor variant may be localized in the larynx, trachea, or nasopharynx.
-
Spindle Cell Carcinoma
Spindle cell carcinoma is a type of cancer characterized by the distinctive morphology of its cells, which are elongated and spindle-shaped. These cells often have an origin in connective and muscular tissues, sometimes classifying them among sarcomas. The most frequently affected areas by this type of cancer include the pharynx, larynx, and oral cavity.
-
Verrucous Squamous Cell Carcinoma
Verrucous squamous cell carcinoma is a distinctive variant of squamous cell carcinoma, characterized by a "verrucous" appearance similar to warts. This characteristic is observed macroscopically in the tumor, giving a specific appearance to these skin lesions.
Head & neck cancer treatments and advances
The treatment of head & neck cancers is determined by several factors, such as the type of cancer, its stage, and the patient's physical condition. The main therapeutic modalities include:
-
Surgery: Often employed when the tumor is accessible, surgery involves interventions such as pharyngectomy (removal of the pharynx), laryngectomy (removal of the larynx and vocal cords), or glossectomy (removal of the tongue).
-
Radiotherapy: For head & neck cancers, radiotherapy, involving the irradiation of the tumor, can be as effective as surgery. It may be prescribed in the absence of surgery or chemotherapy.
-
Chemotherapy: Using anticancer drugs, chemotherapy acts on cancer cells but can also affect other cells, leading to side effects. It may be considered after surgery or radiotherapy.
-
Targeted Therapies: Targeting specific abnormalities in cancer cells, targeted therapies, such as cetuximab, are beginning to be used for head & neck cancers.
-
Immunotherapy is not yet an established protocol for head & neck, but it is currently under study in clinical trials.
It is important to note that the choice of treatment is personalized based on the specific characteristics of each case, and decision-making requires a thorough evaluation of the patient's clinical situation.

Additional resources


