Home › Biological sample › Cancer › Thyroid
Thyroid cancer biological samples
For Translational Research
The development of drugs and diagnostic tests for the treatment and detection of thyroid cancer requires conducting studies on biological samples obtained from patients with thyroid cancer.
A brief overview of the various types of thyroid cancer and how the services offered by Labtoo contribute to accelerating research and development projects in the pharmaceutical industry.

Biospecimen from thyroid cancer patients
Tissues from thyroid cancer patients (tumoral & normal adjacent)
Fresh resection & biopsy
Frozen samples (OCT & FF)
FFPE blocks & slides
Blood derivatives from thyroid cancer patients
-
Whole Blood
-
PBMC
-
Plasma
-
Serum
Biofluids from thyroid cancer patients
-
Thyroid FNA rinse fluid
-
Urine
-
Saliva
-
Other
Associated clinical data from thyroid cancer patients
-
Age
-
Gender
-
TNM Classification
-
Undergone Treatment
-
Medical Imaging
-
HIV/HBV/HCV status
-
Mutations
-
Other Data (upon request)
Send your request to our team:
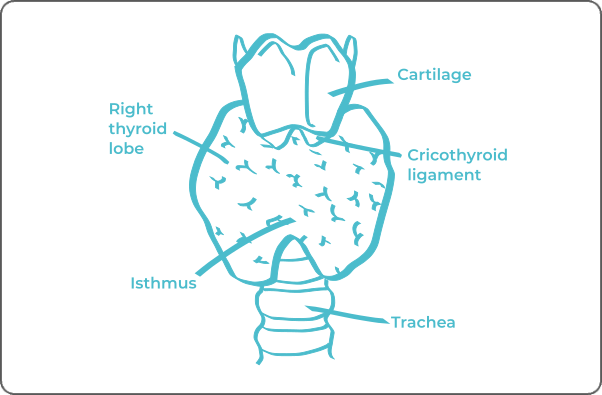
What are thyroid tumors?
The majority of thyroid carcinomas originate from thyrocytes, specialized cells that constitute the functional units of the thyroid, known as thyroid follicles, responsible for synthesizing thyroid hormones.
The classification of thyroid carcinomas is based on their histological differentiation, dividing these cancers into two major categories:
Differentiated carcinomas
Accounting for 90% of cases, these tumors exhibit morphology and function similar to normal thyroid cells.
This category can be further subdivided into two subtypes based on their microscopic appearance: papillary carcinomas and follicular carcinomas
Undifferentiated carcinomas
Also known as anaplastic carcinomas, these tumors are characterized by chaotic cellular behavior, imparting greater aggressiveness and increased therapeutic resistance compared to differentiated carcinomas.
| Type of Thyroid Cancer | Cell of Origin | Frequency |
|---|---|---|
| Papillary Carcinoma | Follicular Cell | ≈ 80% |
| Follicular Carcinoma | Follicular Cell | ≈ 10% |
| Medullary Carcinoma | C Cell (Parafollicular) | > 5% |
| Anaplastic Carcinoma | Follicular Cell (Poorly Differentiated) | > 2% |
| Other Cancer | Muscular, Lymphatic, Other Cells | > 5% |
A less common third group includes medullary carcinomas, arising from C cells (parafollicular cells) normally responsible for producing calcitonin, which participates in the regulation of calcium in the body.
Thyroid carcinomas demonstrate the ability to metastasize to other organs or adjacent lymph nodes, a phenomenon referred to as metastasis. This characteristic involves the progression of the disease beyond the thyroid, significantly impacting clinical management and therapeutic strategies considered.

Explore Labtoo's Service for Your Biological Sample Research
Labtoo assists you in sourcing biological samples from thyroid cancer patients. Our team manages the entire project of transferring biological materials from inception to sample delivery.
- Feasibility assessment of sample availability or clinical collection from referenced clinical centers
- Validation of regulatory aspects
- Establishment of a contractual framework
- Dispatch of desired samples under appropriate conditions
- Transfer of associated clinical data
- Additional analytical and experimental services
The stages and grades of thyroid cancer
The stage and grade of cancer are commonly used together to provide a comprehensive assessment of the disease and guide optimal treatment.
The determination of cancer stage primarily relies on the TNM classification, which evaluates the tumor size (T), involvement of lymph nodes by cancer cells (N), and the presence of metastases in other parts of the body (M). Concurrently, the grade provides an indication of the degree of differentiation of cancer cells.
Regarding grades, denoted from 1 to 3, Grade G1 indicates well-differentiated cells resembling normal cells, Grade G2 represents moderately differentiated cells, and Grade G3 indicates poorly differentiated cells, suggesting faster and potentially more aggressive growth.
For thyroid cancer, the stages are defined as follows:
Stage I
The tumor is located in the thyroid only and does not measure more than 4 cm.
Stage II
Either the tumor measures more than 4 cm and may have invaded the neck muscles
Or it has spread to nearby lymph nodes, can be any size, and may have invaded the neck muscles.
Stage III
The tumor has invaded one of these parts of the body: the larynx, the soft tissue under the skin, the trachea, the esophagus, or the laryngeal nerve.
The tumor may also have spread to nearby lymph nodes.
Stage IV A
Invasion of the connective tissue of the spine, blood vessels of the mediastinal space, or the region surrounding the carotid artery.
Possible invasion of nearby lymph nodes.
Stage IV B
Spread of the tumor to other parts of the body such as the lungs, liver, or bones.
The cancer becomes metastatic.
Rare forms of thyroid cancer
It happens that rarer forms of thyroid cancer develop, among which are:
-
Thyroid Lymphoma
Considered a non-Hodgkin lymphoma, this is a cancer of the lymphatic tissue that can develop in the thyroid.
-
Thyroid Sarcoma
A very rare cancer that develops from the connective tissues of the thyroid.
-
Mucoepidermoid Carcinoma
An infrequent cancer characterized by the presence of mucous and epidermoid cells.
Thyroid cancer treatments and advances
The treatment of thyroid cancer depends on the type of cancer, its stage, and the patient's physical condition. The main therapeutic modalities for managing the condition are:
-
Surgery: Surgery is often considered for thyroid cancers. It may involve resecting part of the thyroid (lobectomy) or the entire thyroid (total thyroidectomy). Depending on the tumor's advancement, the surgeon will often remove all lymph node chains around the neck.
-
Radiotherapy: Iodine-131 radiotherapy is a method that can be used after surgery to eliminate any remaining cancer cells. This method may not be recommended for all types of thyroid cancer.
-
Hormone Therapy: The removal of the thyroid gland necessitates hormone therapy to compensate for hormone deficiencies. In this context, hormone therapy is not aimed at eliminating cancer cells.
-
Chemotherapy: It is not the most commonly used method after surgery. However, it may be employed in cases of anaplastic thyroid cancer.
-
Targeted Therapies: These medications target specific anomalies present in cancer cells. They are used when specific genetic mutations are identified. Targeted therapies may be considered, especially for certain subtypes of thyroid cancer.
Immunotherapy is not yet widely adopted in cases of thyroid cancer.

Additional resources

Life cycle of human biological sample

Drug development

Endocrine disorders