Home › Biological sample › Cancer › Bladder
Bladder cancer biological samples
For research applications
The development of drugs and diagnostic tests for the treatment and detection of bladder cancer requires conducting studies on biological samples obtained from patients with bladder cancer.
A brief overview of the various bladder cancer types and how the services offered by Labtoo contribute to accelerating research and development projects in the pharmaceutical industry.

Biospecimen from bladder cancer patients
Tissues from bladder cancer patients (tumoral & normal adjacent)
Fresh resection & biopsy
Frozen samples (OCT & FF)
FFPE blocks & slides
Blood derivatives from bladder cancer patients
-
Whole Blood
-
PBMC
-
Plasma
-
Serum
Biofluids from bladder cancer patients
-
Urine
-
Other
Associated clinical data from bladder cancer patients
-
Age
-
Gender
-
TNM Classification
-
Undergone Treatment
-
Medical Imaging
-
HIV/HBV/HCV status
-
Mutations
-
Other Data (upon request)
Send your request to our team:
What are bladder tumors?
Cancerous bladder tumors are often classified based on their stage of advancement, indicating the extent of tumor invasion into layers beyond the original. The distinctions are as follows:
Non-invasive tumors
Also referred to as superficial tumors or NMIBC (Non-Muscle-Invasive Bladder Cancer), these tumors remain at the urothelium cell level and do not extend into the muscular cells of the bladder.
Invasive tumors
Or MIBC (Muscle-Invasive Bladder Cancer), representing more severe cases. In this context, tumors have infiltrated the muscular cells, significantly increasing the likelihood of metastasis.
| Type of Bladder Cancer | Origin Cells | Frequency |
|---|---|---|
| Urothelial Carcinoma (or Transitional) | Urothelial Cells | ≈ 90% |
| Squamous Cell Carcinoma | Squamous Cells | 3 - 8% |
| Adenocarcinoma | Glandular Cells | 1 - 2% |
| Neuroendocrine Carcinoma | Neuroendocrine Cells | > 1% |
| Sarcoma | Mesenchymal Cells | > 1% |
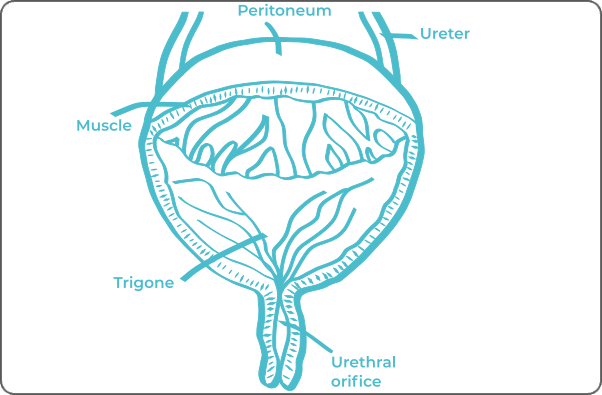
The vast majority of bladder cancers (90%) are urothelial carcinomas, or transitional cell carcinomas. These tumors originate from cells lining the interior of the bladder (the uterine mucosa).
In rare cases of invasive tumors extending beyond the inner lining, the cancer may consist of various cell types intermingled with urothelial cancer cells. This phenomenon is termed divergent differentiation, and the most commonly found cells are squamous cells (squamous cell carcinomas) and glandular cells (adenocarcinoma).
Bladder cancer can be metastatic, categorized as Stage IV. Most commonly, metastases from the bladder migrate to lymph nodes, liver, lungs, and bones.
Explore Labtoo's Service for Your Biological Sample Research
Labtoo assists you in sourcing biological samples from bladder cancer patients. Our team manages the entire project of transferring biological materials from inception to sample delivery.
- Feasibility assessment of sample availability or clinical collection from referenced clinical centers
- Validation of regulatory aspects
- Establishment of a contractual framework
- Dispatch of desired samples under appropriate conditions
- Transfer of associated clinical data
- Additional analytical and experimental services
The stages and grades of bladder cancer
The stage and grade of cancer are commonly used together to provide a comprehensive assessment of the disease and guide optimal treatment.
The determination of cancer stage primarily relies on the TNM classification, which evaluates the tumor size (T), involvement of lymph nodes by cancer cells (N), and the presence of metastases in other parts of the body (M). Concurrently, the grade provides an indication of the degree of differentiation of cancer cells.
Regarding grades, denoted from 1 to 3, Grade G1 indicates well-differentiated cells resembling normal cells, Grade G2 represents moderately differentiated cells, and Grade G3 indicates poorly differentiated cells, suggesting faster and potentially more aggressive growth.
For bladder cancer, the stages are defined as follows:
Stage 0
The tumor is confined to the lining of the bladder, termed "carcinoma in situ."
Stage I
The tumor has invaded the connective tissue layer of the bladder.
Stage II
The tumor has penetrated the muscular layer of the bladder, becoming invasive.
Stage III A
The tumor has invaded tissues adjacent to the bladder outside, without reaching the pelvic or abdominal wall. Alternatively, the cancer has spread to a lymph node in the pelvic region.
Stage III B
The cancer spread to at least 2 lymph nodes in the pelvic region or at least 1 lymph node above the pelvic region.
Stage IV A
Invasion of cancer into the pelvic or abdominal wall or invasion of the farthest lymph nodes from the bladder.
Stage IV B
Presence of metastases in other parts of the body, such as the liver, bones, or lungs.
Rare forms of bladder cancer
Occasionally, rarer forms of bladder cancer may develop, among which are:
-
Squamous Cell Carcinoma
This type of cancer originates from flat cells of the epithelium.
-
Adenocarcinoma
A cancer that forms from glandular cells of the bladder.
-
Small Cell Carcinoma
A cancer taking shape in the neuroendocrine cells of the bladder.
-
Sarcoma
Cancer that develops in soft tissue cells. In the case of the bladder, leiomyosarcomas are most commonly found in adults, while rhabdomyosarcomas are more prevalent in children.
Bladder cancer treatments and advances
The primary treatment for bladder cancer typically involves surgical intervention, with tumor removal in cases of non-invasion or, in more advanced cases, bladder resection along with adjacent structures, such as the prostate in men or the uterus and urethra in women. Additional procedures, including chemotherapy, immunotherapy, or radiotherapy, may be considered depending on the severity of the disease.
Recent advancements in bladder cancer treatment have focused on targeted therapies, an approach that directly targets specific molecules present in tumors. Among these breakthroughs, antibody-drug conjugates stand out. These medications merge a monoclonal antibody with a chemotherapeutic substance.
The antibodies are designed to selectively bind to proteins on the surface of cancer cells, facilitating the internalization of the cytotoxic substance and the targeted destruction of cancer cells.

Additional resources


